(2) A study of the relative effectiveness of 3 different anorexiants in 95 obese patients has provided a practical illustration of the usefulness of the system in the conduct of clinical investigations under conditions of general practice.
Southern Medical Journal. 56(6):650-653, June 1963.
BUTTERY, CHRISTOPHER M.G. M.D.
Clinical Investigation in General Practice: The Use of a Simplified Data- Recording System.
If there is interest, the family physician could contribute much to the advance of clinical information. He has the advantages of long-term follow-up denied the university physician. The key-sort cards described here make for an accurate method of assembling statistics and can be used in a doctor's office with less expenditure of time than usual records.
THE EVER-INCREASING number of new drugs reaching the market makes it increasingly difficult for the physician to be sure he is selecting the most appropriate drug for each individual patient. Most of those engaged in the general practice of medicine are content to leave clinical investigation to the university centers on the supposition that the circumstances of general practice preclude them from having either the time or the facilities for drug research. I hold that this supposition is not entirely valid. It is obviously impossible for any physician, with or without teaching hospital affiliation, to evaluate the entire gamut of modern drugs. However, most general practitioners have special areas of interest, and it seems feasible to me that they may carry out simple clinical evaluations and studies within their particular sphere of interest provided a simple time-saving method of recording clinical data is employed. The pursuit of clinical research by the general practitioner will be found to be both intellectually stimulating and of enormous practical value in prescribing for his patients. This last point is lent special emphasis since patients presenting themselves for treatment at university centers can scarcely be regarded as representative of those consulting general practitioners, because in most instances they have been funneled from the generalist to the internist and thence to the university. It follows that research findings in such patients are not necessarily applicable in toto to the average patient approaching the general practitioner for treatment.
In my general practice I make my ownclinical investigation of drugs within especial spheres of interest, including particularly arthritis and psychiatric disturbances. The key to my system is the collection of clinical data on specially prepared key-sort punch cards which may be obtained from Royal McBee, Inc. The recording of data following each examination takes but a few moments, and at the conclusion of a clinical study the cards may readily be sorted in a manner to provide accurate statistical data, not only on degree of effectiveness, but also on a wide range of correlated factors.
The purpose of this report is to give a brief description of this system, using as an example the relative effectiveness of 3 appetite suppressants in controlling obesity
Description of Cards
A reproduction of the McBee card is presented in figure 1. The card has a series of perforations along each edge. Each of the perforations is related to a specific procedure or finding, the nature of which is printed adjacent to' e appropriate perforation. Thus, for example, one perforation may relate to spinal tap. When the patient receives a spinal tap this particular perforation is clipped cm his card in such a manner that it becomes a "tooth-gap" extending to the edge of the card. If in a series of patients under study some have received a spinal tap and others have not, the related cards will have either a perforation or tooth-gap at the point marked "spinal tap." When the cards are placed in a stack a spear is passed through the designated perforation. The mixed perforations and tooth-gaps will selectively hold those with intact perforations. The cards with tooth gaps can be extracted and represent the cards relating to patients who had spinal taps, they are segregated for study at the cost of only a moment's work. Obviously, the number of further subdivisions that can be made is limited only by the number of perforations on the card. Thus, a multitude of factors can be determined and correlated one with another.
In the center of the card, space may be provided for the patient's name and other pertinent data which it is not contemplated shall be the subject of statistical analysis since these items are not key-punched.
The usefulness of these cards is not confined to formal clinical investigation. By making out a card for each main complaint and stacking the cards numerically, in accordance with the number on each patient's file, the physician may, for example, rapidly determine the results he has previously obtained with any particular drug or procedure.
The specific design of the card is a matter for the individual physician, since both the nature and number of the individual points he wishes to check will depend on his particular interest and the type of investigation he plans to pursue. I employ a card 10" by 8" with the 4 edges being perforated. A card of this size permits 48 perforations on each long side and 40 on each shorter side, providing for a total of 176 different points which can conceivably be checked. Virtually all areas of diagnosis, treatment, and progress can be recorded with this relatively large number of check points. In any specific study only a small proportion of these check points are utilized. The advantage, however, of having a card with a large number of check points is that it may be adapted to almost any type of investigation, thus avoiding the necessity of having to have cards custom-made for each specific study.
Procedure of Study
As an example, in my general practice 95 patients were treated for obesity, and appropriate records were maintained on punch cards by the system described. The purpose of the study was to make an evaluation of 3 anorexiant agents. employed as follows:
Clinical Results
All data necessary for clinical evaluation were segregated by means of the key-sorting system described. Thus, the first step was to segregate from investigation files all the cards related to this particular study. Thereafter, further separations were made progressively according to the degree of weight loss achieved over periods of one week, one month, and 3 months. The various stacks resulting were then further subdivided according to the particular anorexiant employed. The over-all results so obtained are summarized in table 1. Anorexiant III provided the most satisfactory results, with an average weight loss at the end of one month of 19.48 pounds; and at the end of 3 months of 29.18 lbs. The corresponding figures for Anorexiant I were 12.41 and 21.30 pounds, and for Anorexiant II 8.67 and 21.67 pounds.
Commentary
From data obtained by the use of key-sort cards as described it was found that many patients in this study readily lost 3 or more pounds per week without apparent ill effect. Anorexiant III provided more favorable results than the other two. The favorable effect produced in some patients by the addition of a tranquilizer and the institution of appropriate psychotherapy underscores the importance of psychic factors in the causation of obesity.
The study is being continued with a view to coordinating numerous other factors in the development of obesity and its response to treatment.
Summary
(1) A simple system of recording clinical data in readily segregated form b the use of punched key-sort cards has been described.
RECORD OF WEIGHT LOSS IN PATIENTS RECEIVING THREE DIFFERENT TYPES OF ANOREXIANT THERAPY
Weight Loss (lbs.) |
After One Month |
Weight |
After Three Months |
||||
0- 5 |
1 |
2 |
5 |
0- 5 |
1 |
|
|
5-10 |
9 |
3 |
9 |
5-10 |
1 |
|
|
10-15 |
4 |
|
23 |
10-20 |
2 |
3 |
8 |
15-20 |
4 |
1 |
16 |
20-30 |
4 |
2 |
7 |
20-25 |
2 |
|
15 |
30-40 |
2 |
|
12 |
25+ |
|
|
1 |
40+ |
- |
|
10 |
TOTALS |
20 |
6 |
69 |
|
10 |
6 |
38 |
![]()
(2) A study of the relative effectiveness of 3 different anorexiants in 95 obese patients has provided a practical illustration of the usefulness of the system in the conduct of clinical investigations under conditions of general practice.
The figs below provides an overview of the punch card which was intended to allow me to assess the effectiveness of my practice and plan continuing education, as well as track several areas of importance for research in general office practice. Research in office practice was not established until the 1970s in the US although it was a common practice in the UK.
Punch card designed in 1956 showing two punched areas.
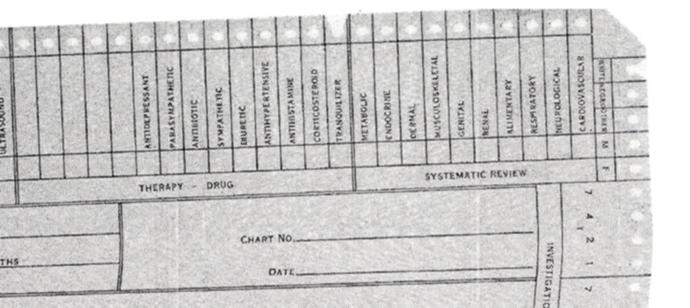
Section of punch card showing therapy choices. In the 1956 when this card was designed there were only about 35 to 40 drugs that were useful and validated in general practice. The systematic reviewed allowed m\e to ensure that all patents eventually got a complete systems review.
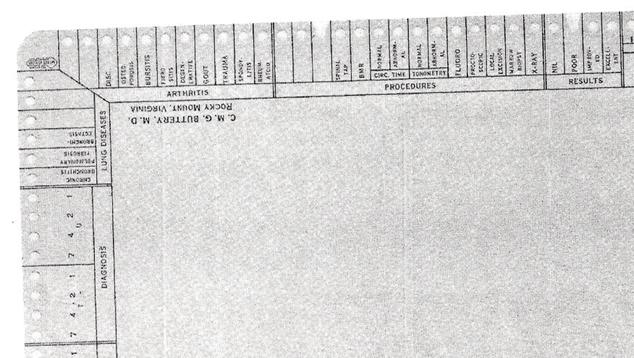
This section of the card allowed me to focus in my research interests and analyze the procedures used in my practice as well as performing a simple assessment of outcome of treatment..